NY DOH-5032 2011-2025 free printable template
Show details
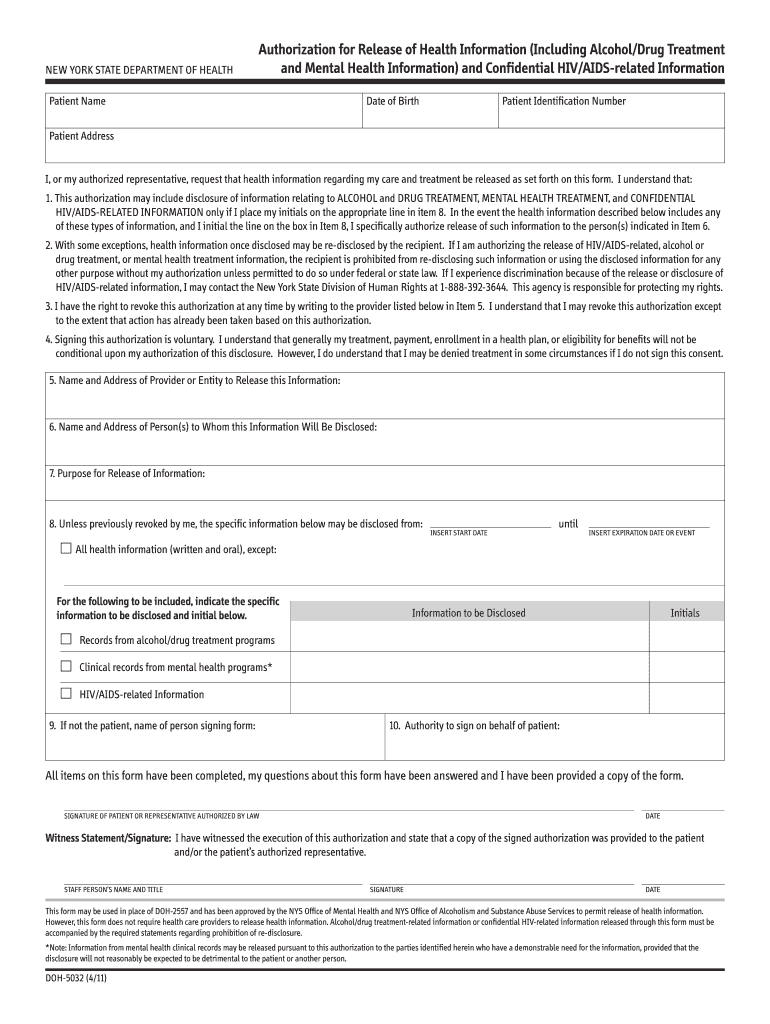
STAFF PERSON S NAME AND TITLE SIGNATURE This form may be used in place of DOH 2557 and has been approved by the NYS Office of Mental Health and NYS Office of Alcoholism and Substance Abuse Services to permit release of health information. However this form does not require health care providers to release health information. Alcohol/drug treatment related information or confidential HIV related information released through this form must be accompanied by the required statements regarding...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign pdffiller form
Edit your doh 5032 download form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your doh 5032 form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit obtain the ny doh 5032 form from the new designated fields including name address and contact details online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Log in to account. Start Free Trial and sign up a profile if you don't have one yet.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit doh form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
With pdfFiller, dealing with documents is always straightforward. Now is the time to try it!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out nys hippa release form
How to fill out NY DOH-5032
01
Obtain the NY DOH-5032 form from the New York State Department of Health website or local health department.
02
Fill out the applicant's information in the designated fields, including name, address, and contact details.
03
Provide detailed information about the facility or location relevant to the application.
04
Clearly indicate the purpose of the application in the appropriate section.
05
Attach any required documents that support your application.
06
Review the form for completeness and accuracy.
07
Submit the completed form to the appropriate health department office as instructed.
Who needs NY DOH-5032?
01
Individuals or organizations seeking to operate a specific type of health-related facility in New York State.
02
Professionals and entities needing to report information as mandated by the New York State Public Health Law.
03
Healthcare providers applying for permits or licenses related to health services.
Fill
form
: Try Risk Free
People Also Ask about
Should I decline HIPAA authorization?
Should I sign this “HIPAA Authorization” for release of my medical records? No, you should not sign the HIPAA authorization for the release of your medical records. Often, the insurance company will act as though they cannot begin to decide how much money to offer you until they have all of your medical records.
What is HIPAA authorization in the consent form?
A HIPAA consent form is a legal document that authorizes covered entities to disclose protected health information that is not permitted by the HIPAA Privacy Rule. The form must be retained as proof that the authorization was obtained in writing to waive certain Privacy Rule restrictions.
What is HIPAA authorization?
A HIPAA authorization is consent obtained from an individual that permits a covered entity or business associate to use or disclose that individual's protected health information to someone else for a purpose that would otherwise not be permitted by the HIPAA Privacy Rule.
How do I fill out a HIPAA form?
1:05 2:54 HIPAA Release Form Instructions - YouTube YouTube Start of suggested clip End of suggested clip But you can name additional people in there as well. Starting at the top you will want to clearlyMoreBut you can name additional people in there as well. Starting at the top you will want to clearly print your full name in the space provided. Along with your address. And social security number.
What is a HIPAA release form?
A HIPAA authorization form gives covered entities permission to use protected health information for purposes other than treatment, payment, or health care operations.
What is an example of HIPAA authorization?
I hereby authorize use or disclosure of protected health information about me as described below. I understand that the information used or disclosed may be subject to re-disclosure by the person or class of persons or facility receiving it, and would then no longer be protected by federal privacy regulations.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I edit NY DOH-5032 from Google Drive?
Simplify your document workflows and create fillable forms right in Google Drive by integrating pdfFiller with Google Docs. The integration will allow you to create, modify, and eSign documents, including NY DOH-5032, without leaving Google Drive. Add pdfFiller’s functionalities to Google Drive and manage your paperwork more efficiently on any internet-connected device.
How do I fill out the NY DOH-5032 form on my smartphone?
The pdfFiller mobile app makes it simple to design and fill out legal paperwork. Complete and sign NY DOH-5032 and other papers using the app. Visit pdfFiller's website to learn more about the PDF editor's features.
How do I edit NY DOH-5032 on an Android device?
You can. With the pdfFiller Android app, you can edit, sign, and distribute NY DOH-5032 from anywhere with an internet connection. Take use of the app's mobile capabilities.
What is NY DOH-5032?
NY DOH-5032 is a form used by the New York State Department of Health for reporting essential information regarding communicable diseases and health conditions.
Who is required to file NY DOH-5032?
Healthcare providers, laboratories, and certain institutions are required to file NY DOH-5032 when they diagnose or identify a reportable communicable disease.
How to fill out NY DOH-5032?
To fill out NY DOH-5032, you need to provide patient demographic information, the diagnosis or condition, relevant clinical information, and any required laboratory results.
What is the purpose of NY DOH-5032?
The purpose of NY DOH-5032 is to collect critical data on infectious diseases to help control outbreaks and protect public health.
What information must be reported on NY DOH-5032?
Required information includes patient's name, date of birth, address, telephone number, the disease diagnosed, date of diagnosis, and the reporting entity's details.
Fill out your NY DOH-5032 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
NY DOH-5032 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
